
 Get More Help in Nevada
Get More Help in NevadaDental & Oral Health Screening
Guidance on screening for dental health issues in children and adolescents

Oral health screening by the primary care clinician is an important part of comprehensive well-child care. Oral health affects eating habits, sleep, smiling, social interactions, and the child's overall health. In addition, poor oral health increases the risks of developing problems with drinking, eating, and speaking for children with special health care needs. [Weckwerth: 2016] Because infants and young children usually have several visits with their medical home before ever seeing a dentist, the primary care clinician is often the first person to recognize and address their oral health needs; >20% of children ages 2-11 have untreated dental caries that could be identified in the medical home. [National: 2018] Caries can cause pain and increase the risk of systemic infections.
Key Points
Screen early
Oral health screening provided by the primary medical provider
includes a caries risk assessment, anticipatory guidance to prevent disease, and
referral to a dental home, which is essential to every well-child visit.
Dental home
Establish a dental home by 12 months old or earlier, starting at 6
months old based on risk and/or 6 months after the first tooth eruption.
Fluoride
Supplemental fluoride is recommended for those without adequate
fluoride in community water supply. [Krol: 2023]
Guidelines
Davidson K.
Prevention of dental caries in children younger than 5 years: screening and interventions.
JAMA. 2021; https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/pr...
Krol DM, Whelan K.
Maintaining and Improving the Oral Health of Young Children.
Pediatrics.
2023;151(1).
PubMed abstract
Bright Futures.
Promoting oral health: implementation tip sheet.
Guidelines for Health Supervision of Infants, Children, and Adolescents, 4th Edition.
2020.
/ Full Text
American Academy of Pediatric Dentistry.
Antibiotic prophylaxis for dental patients at risk for infection.
The Reference Manual of Pediatric Dentistry..
2022;Chicago, Ill:500-6.
/ Full Text
Screening and Assessment
The American Academy of Pediatrics recommends oral health-related anticipatory guidance to start during prenatal visits and continue at every well-child visit to adulthood. Dental caries risk assessment, fluoride varnish, and fluoride supplement in the medical home start at the 6- and 9-month well-child checks, depending on tooth eruption. [American: 2023] Referral to a pediatric or general dentist should be made at the 6-month well-child visit, with follow-up monitoring at subsequent well-child visits to ensure a dental home is established and utilized.
A caries risk assessment is recommended during the well-child visit if a dental
home is not established or utilized for regular preventive check-ups. [Centers: 2004] The Oral Health Risk Assessment Tool (AAP) ( 302 KB) provides a brief
questionnaire about risk factors, protective factors, and clinical findings
(photos are included for reference) to establish an action plan and
self-management goals.
302 KB) provides a brief
questionnaire about risk factors, protective factors, and clinical findings
(photos are included for reference) to establish an action plan and
self-management goals.
For children who receive oral health screening from programs like Early Intervention, the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), or Early Head Start, medical homes may choose to limit screening to questions about feeding problems, but should continue with anticipatory guidance including feeding habits. (Listings for these programs can be found below under Referrals and Services.)
Anticipatory Guidance
Primary care clinicians can help prevent dental-related diseases in children by providing anticipatory guidance to parents, guardians, families, and children. [Clinical: 2016] Oral health anticipatory guidance starts at prenatal visits and continues through adulthood.
Common guidance includes:
- Wipe the infant's gums and tongue with a wet cloth after feeding.
- Brush your child's teeth
twice daily using fluoride toothpaste.
- Once teeth erupt, all children <3 years old should use a smear of fluoride toothpaste (about the size of a grain of rice), and older children should use a pea-sized amount.
- Children need help brushing their teeth until they can do it well enough by themselves (usually about 8 years old).
- Floss daily.
- All family members should see a dentist twice a year for preventive care and cleaning, including professional cleaning.
- Bottles and sippy cups should not be propped or left with infants when caregivers are not actively feeding the child.
- Once teeth erupt, avoid nursing or feeding at night because the milk remaining in the mouth can lead to caries. The caregiver can offer water if the older infant or child is thirsty at night.
- Wean from bottle feeding by age 12 months.
- Discourage thumb-sucking after age 4 or 5 years.
- Provide healthy snacks (e.g., cheese, fruit, and vegetables).
- Prevent frequent snacking on sugar- and carbohydrate-containing foods.
- Minimize juice consumption to 0-6 ounces per day of 100% fruit juice; avoid soda, energy drinks, and other sweetened beverages.
- Drink and cook with fluoridated tap water if available.
- Consider fluoride mouthwash for children ≥6 years old. [Council: 2013]
For older children, also discuss:
- Reducing or eliminating consumption of energy drinks and sweetened beverages
- Wearing a mouth guard during contact sports
- Detrimental effects of smoking/tobacco use
- Detrimental effects of illegal drugs, including methamphetamines
- Detrimental effects of oral piercings
- Oral-related infections, including the risk of sexually transmitted illnesses that can affect the lips, mouth, and throat

Fluoride
Fluoride acts in 3 important ways to prevent caries: 1) by strengthening enamel, 2) by remineralizing enamel, and 3) by affecting microbial metabolism and reducing acid production by cariogenic bacteria. Systemic, fluoride in water or by supplement, and topical fluoride applications are the primary sources of fluoride. [American: 2021]
The U.S. Preventive Services Task Force (USPSTF) recommends clinicians prescribe oral fluoride supplementation starting at age 6 months for children whose water supply is deficient in fluoride (<0.6 ppm Fl) and that clinicians apply fluoride varnish to the primary teeth of all infants and children starting at the age of primary tooth eruption (Grade B). All children 5 years and younger deserve to have the application of fluoride varnish (5% sodium fluoride) as part of health maintenance and preventive care. Fluoride varnish application should be a covered benefit and separately paid service (i.e., not considered incidental to the office visit). [Clark: 2020]
Higher-risk children may require more frequent fluoride varnish. For example, consider more frequent topical fluoride applications in the medical home for children with uncontrolled gastric reflux, as this can increase sensitivity and erode enamel. The table below from [Clark: 2020] provides condensed recommendations for fluoride modalities in patients with low and high caries risk.
Fluoride for Low- and High-Risk Patients [Clark: 2020]
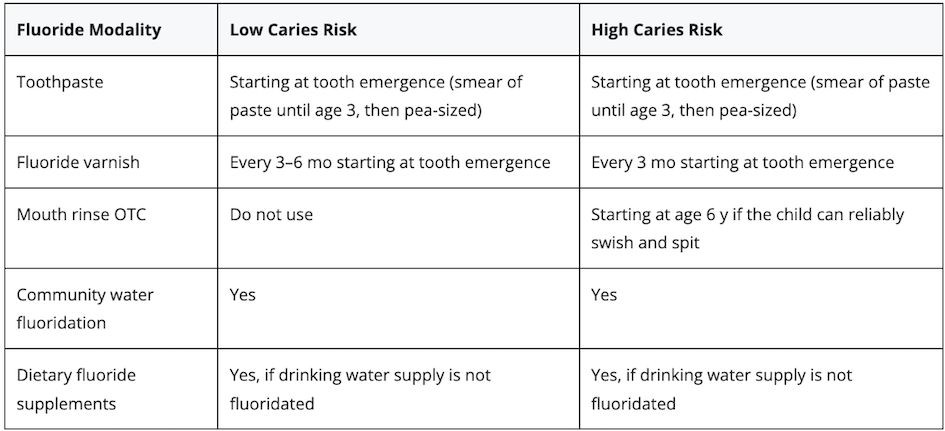
Supplemental fluoride is essential to the development of teeth and the prevention of tooth decay. Community-based fluoridated water levels may vary from county to county, so water fluoride levels must be verified before subscribing to supplements. If the level is unknown (such as in well water), it should be tested to determine if supplementation is needed. [American: 2023] Fluoride content of water supplies in the United States can be found at My Water's Fluoride (CDC).
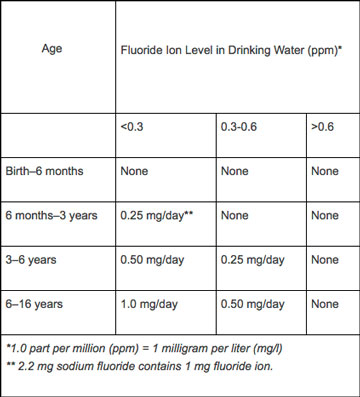
Oral fluoride supplements for children ages 6 months to 16 years are recommended for children with suboptimal fluoridated water intake (consider drinking water, cooking water, water at school, etc.). [American: 2023] Supplementation of fluoride and vitamin D during the first year of life is associated with fewer cavities in the primary teeth. [Kühnisch: 2016] Although recommendations are from 2010, the table to the left still provides current supplementation information. Calcium and Vitamin D has information about supplementation for children.
Dental fluoride varnish should be placed approximately every 6 months by the medical or dental clinician. If in the medical home, administration of the varnish may be performed by trained staff, such as a medical assistant or nurse. A 1-hour online course, with continuing medical education credits available, can be found at Oral Health Curriculum (Smiles for Life). For more information about fluoride, see The Debate Over Fluoridated Water (AAP).
Dental Home
The medical home should talk with families about establishing a dental home by 12 months of age (and as early as 6 months of age). [American: 2005] A dental home is a primary care dental provider with a comprehensive and up-to-date approach for preventing dental problems, providing anticipatory guidance about dental issues and nutrition and behaviors that affect dental care, assessing for adequate fluoride and prescribing supplements when indicated, administering topical fluoride applications, assessing and treating dental issues, placing sealants for high-risk children, and referring to dental specialists as needed for surgery or orthodontics. [EQIPP: 2017] The primary care clinician should assist parents with identifying an appropriate pediatric or general dentist office, keeping in mind the child’s age, health conditions, and behavior. The dental office’s participation with dental insurance carriers varies greatly and should be considered when making a referral.
Referrals and Services
Early Intervention for Children with Disabilities/Delays
(see NV providers
[30])
Early intervention (EI) are services provided through a family
coaching method to help children with disabilities or delays meet goals in areas
of development.
WIC Assistance
(see NV providers
[54])
Provides nutrition and breastfeeding services and supplemental
foods to pregnant women, mothers, infants, and children up to their 5th
birthday.
Head Start/Early Head Start
(see NV providers
[66])
Head Start provides comprehensive education, health, nutrition,
and family services to poverty-level children and their families. Local grantees
receive federal funding for Head Start (HS), Migrant/Seasonal Head Start (MSHS),
and Early Head Start (EHS) programs, the latter serving children from birth to
age three and expectant mothers.
Healthcare, Dental > …
(see NV providers
[33])
A directory of providers, addresses, and contact information.
Patient Education
Infective Endocarditis? (AHA)
A fact sheet about this condition and the importance of treatment;
American Heart Association.
Resources
Information & Support
Related Portal Content
For Professionals
Open Wide: Oral Health Training for Professionals (USDA)
Series of 4 web-based, self-study modules to help health and early childhood professionals to promote oral health. The modules
have information about tooth decay, risk factors, and prevention; explain how to perform an oral health risk assessment and
oral health screening; and highlight anticipatory guidance to share with parents; WIC and Works Resource System, U.S. Department
of Agriculture.
Online Fluoride Varnish Training (SFL)
A 1-hour, free course to train medical home providers on how and when to administer fluoride varnish and other care. This
is within the Access the Caries Risk Assessment, Fluoride Varnish, and Counseling module. Continuing medical education credits
available; Smiles for Life National Oral Health Curriculum.
Oral Health Anticipatory Guidance List (Bright Futures)
A brief list of anticipatory guidance items for children from birth to young adulthood.
Community Water Fluoridation FAQs (CDC)
Information about guidelines, scientific reports, and frequently asked questions about fluoride in wells and bottled water;
Centers for Disease Control and Prevention.
For Parents and Patients
Campaign for Dental Health (AAP)
Created to ensure that people of all ages have access to the most effective, affordable, and equitable way to protect teeth
from decay; American Academy of Pediatrics.
First Dental Visit (Stanford Medicine)
Discusses why dental exams are important for children, how they are performed, and what to expect from the assessment.
The Debate Over Fluoridated Water (AAP)
Pros, cons, facts, and myths about fluoride; American Academy of Pediatrics.
Tools
My Water's Fluoride (CDC)
A user-friendly, searchable database that allows consumers to learn about the fluoride levels in their drinking water; Centers
for Disease Control and Prevention.
Oral Health Pocket Guide (Bright Futures)
Anticipatory guidance information, risk assessment guides, a fluoride supplement chart, and tools for improving the oral health
of children from before birth to young adulthood.
Oral Health Practice Tools (AAP)
Many tools in Spanish and English to help with setting up your practice to include oral health, applying fluoride varnish,
performing a risk assessment and an oral exam, helping families find a dental home, and providing patient education; American
Academy of Pediatrics.
Oral Health Risk Assessment Tool (AAP) ( 302 KB)
A PDF to aid in the implementation of oral health risk assessment during health supervision visits. Contains photos and a
brief questionnaire about risk factors, protective factors, and clinical findings; American Academy of Pediatrics.
Services for Patients & Families in Nevada (NV)
| Service Categories | # of providers* in: | NV | NW | Other states (3) (show) | | NM | RI | UT |
|---|---|---|---|---|---|---|---|---|
| Early Intervention for Children with Disabilities/Delays | 30 | 3 | 34 | 13 | 51 | |||
| General Dentistry | 13 | 1 | 12 | 47 | 93 | |||
| Head Start/Early Head Start | 66 | 10 | 18 | 26 | ||||
| Healthcare, Dental | 33 | 2 | 16 | 66 | 150 | |||
| Oral/Maxillofacial Surgery | 2 | 1 | 2 | 5 | ||||
| Orthodontics | 4 | 3 | 17 | |||||
| Pediatric Dentistry | 24 | 2 | 6 | 54 | 50 | |||
| WIC Assistance | 54 | 13 | 42 | |||||
For services not listed above, browse our Services categories or search our database.
* number of provider listings may vary by how states categorize services, whether providers are listed by organization or individual, how services are organized in the state, and other factors; Nationwide (NW) providers are generally limited to web-based services, provider locator services, and organizations that serve children from across the nation.
Page Bibliography
American Academy of Pediatric Dentistry.
Antibiotic prophylaxis for dental patients at risk for infection.
The Reference Manual of Pediatric Dentistry..
2022;Chicago, Ill:500-6.
/ Full Text
American Academy of Pediatric Dentistry.
Policy on use of fluoride. The Reference Manual of Pediatric Dentistry.
Chicago: American Academy of Pediatric Dentistry.;
2021.
https://www.aapd.org/media/policies_guidelines/p_fluorideuse.pdf
American Academy of Pediatric Dentistry Council on Clinical Affairs.
Policy on the dental home.
Pediatr Dent.
2005;27(7 Reference):18-9.
PubMed abstract / Full Text
American Academy of Pediatrics.
2023 Recommendations for Preventive Pediatric Health Care.
Pediatrics.
2023;151(4).
PubMed abstract / Full Text
American Dental Association.
Fluoride: Topical and Systemic Supplements.
(2023)
https://www.ada.org/en/resources/research/science-and-research-institu.... Accessed on Fe2, 2024.
Bright Futures.
Promoting oral health: implementation tip sheet.
Guidelines for Health Supervision of Infants, Children, and Adolescents, 4th Edition.
2020.
/ Full Text
Centers for Disease Control & Prevention.
The National Health and Nutrition Examination Survey (NHANES).
National Institute of Dental and Craniofacial Research. 2004; https://www.nidcr.nih.gov/DataStatistics/FindDataByTopic/DentalCaries/...
Clark MB, Keels MA, Slayton RL.
Fluoride use in caries prevention in the primary care setting.
Pediatrics.
2020;146(6).
PubMed abstract / Full Text
Clinical Affairs Committee.
Guideline on Antibiotic Prophylaxis for Dental Patients at Risk for Infection.
Pediatr Dent.
2016;38(6):328-333.
PubMed abstract / Full Text
Council on Clinical Affairs.
Guideline on caries-risk assessment and management for infants, children, and adolescents.
Pediatr Dent.
2013;35(5):E157-64.
PubMed abstract / Full Text
Davidson K.
Prevention of dental caries in children younger than 5 years: screening and interventions.
JAMA. 2021; https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/pr...
EQIPP.
Oral Health Online Course.
2017; American Academy of Pediatrics; https://www.aap.org/EQIPP-Oral-Health-Best-Practices
Krol DM, Whelan K.
Maintaining and Improving the Oral Health of Young Children.
Pediatrics.
2023;151(1).
PubMed abstract
Kühnisch J, Thiering E, Heinrich-Weltzien R, Hellwig E, Hickel R, Heinrich J.
Fluoride/vitamin D tablet supplementation in infants-effects on dental health after 10 years.
Clin Oral Investig.
2016.
PubMed abstract
National Institute of Dental and Craniofacial Research.
Dental caries in children (age 2 to 11).
National Institutes of Health; (2018)
https://downloads.aap.org/AAP/PDF/oralhealth_RiskAssessmentTool.pdf. Accessed on Feb 2, 2024.
Weckwerth SA, Weckwerth GM, Ferrairo BM, Chicrala GM, Ambrosio AM, Toyoshima GH, Bastos JR, Pinto EC, Velasco SR, Bastos RS.
Parents' perception of dental caries in intellectually disabled children.
Spec Care Dentist.
2016;36(6):300-306.
PubMed abstract