
 Get More Help in Nevada
Get More Help in NevadaTypes of Hearing Loss
This section provides descriptions of different types of hearing loss and disorders briefly discussed in other sections of the Medical Home Portal. This section does not provide an exhaustive description of all types of hearing loss. Diagnosis and management is reviewed in the Hearing Loss and Deafness module. This section includes:
- Sensorineural Hearing Loss
- Conductive Hearing Loss
- Mixed Hearing Loss
- Auditory Neuropathy
- Central Hearing Loss and Central Auditory Processing Disorder
- Unilateral Hearing Loss
- Hereditary Nonsyndromic Hearing Loss
Sensorineural Hearing Loss
Sensorineural hearing loss (SNHL) results from damage to the inner ear (cochlea) or to the nerve pathways from the inner ear to the brain. SHNL is sometimes called “nerve deafness.” The “sensory” part of the name refers to damage to the inner ear. The cochlea is contained in the inner ear, and along it are located hair cells, which are nerve endings that respond to different pitches of sound. The “neural” part of the name refers to damage to the vestibulocochlear nerve, also known as the 8th cranial nerve, the auditory nerve, or the acoustic nerve. The vestibulocochlear nerve transmits messages to the brain regarding sound and balance. SNHL reduces the ability to hear faint sounds; speech that is loud enough to hear may sound muffled or unclear. SHNL is the most common type of hearing loss and usually cannot be medically or surgically corrected. Causes of SNHL in children include:
- Illnesses, including CMV, bacterial meningitis
- Drugs that are toxic to hearing
- Hearing loss that runs in the family (genetic or hereditary)
- Head trauma
- Malformation of the inner ear
- Exposure to loud noise
- Eighth nerve lesions
- Prematurity
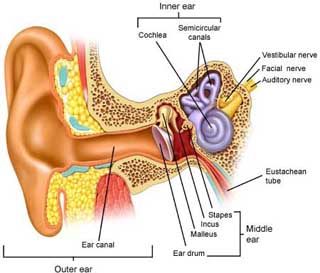
Diagram of the hearing apparatus:
Conductive Hearing Loss
Conductive hearing loss (CHL) occurs when sound is not conducted
efficiently through the outer and middle ear. The middle ear, which includes the
tympanic membrane (eardrum) and ossicles (tiny bones) transmits sounds from the air
environment of the outer ear to the fluid-filled environment of the inner ear. This
transmission process uses the middle ear’s mechanical vibrations to adapt the
impedance of air to the impedance of the fluids in the inner ear. Without a good
impedance match between the two, sound energy is reflected or absorbed rather than
conducted, and a hearing loss occurs. Conductive hearing loss results in inability
to hear faint sounds.
CHL is the most common cause of
hearing loss in childhood and is usually caused by otitis media with effusion (OME).
OME refers to a collection of fluid in the middle ear, which impairs tympanic
membrane function but does not cause acute symptoms of an ear infection. It is
generally a self-limited disorder with most cases resolving spontaneously in in 3-6
months. In a minority of cases, persistent OME may lead to significant hearing loss
and/or tympanic membrane abnormalities, which may ultimately affect permanent
hearing and language development. Other causes of CHL are less common, including
anatomic craniofacial abnormalities, ossicular malformations, foreign body or
cerumen in the external auditory canal, cholesteatoma, and trauma to the tympanic
membrane or middle ear. [Gifford: 2009]
In general, traditional hearing aids work well for
conductive hearing loss. However, some causes of conductive loss can be corrected
medically or surgically. Treatment is individualized, guided by the
otolaryngologist/audiology team. For example, middle ear fluid or Eustachian tube
dysfunction may be resolved with treatment of infection or placement of ventilating
tubes. Other interventions may include foreign body removal, tympanoplasty,
mastoidectomy, or amplification with bone-anchored hearing aids. [Doyle: 2003] In some cases, absence of an outer ear or ear canal
can be surgically repairable, but may require hearing aids for some time. Absence of
the middle ear usually requires permanent use of hearing aids.
Mixed Hearing Loss
Mixed hearing loss describes a condition where a conductive hearing loss occurs in combination with a sensorineural hearing loss (SNHL). This means there is impaired conduction of sound through the outer and middle ear, as well as damage to the cochlea or auditory nerve in the inner ear. Examples in children occur when a child has SNHL and also experiences conductive loss because of otitis media, causing hearing to be poorer than it was from the SNHL alone. Traditional hearing aids can be used with mixed hearing losses. Medical or surgical correction of impaired conduction is typically a focus of treatment in mixed hearing loss.
Auditory Neuropathy
Hearing loss may also be related to a hearing disorder called
auditory neuropathy, or impaired transmission of signals from
the inner ear to the brain, which results in poor speech perception, or disorganized
sounds reaching the brain. Auditory neuropathy typically implies a processing defect
of the auditory (cochlear) portion of the 8th cranial nerve, but similar test
results are found with defective inner hair cells. This type of hearing impairment
is diagnosed when there is an abnormal ABR but a normal OAE result. Variability or
absence of responses to behavioral testing is also an indication of auditory
neuropathy. Because of the wide variability in auditory performance, the term
Auditory Neuropathy Spectrum Disorder (ANSD) was adopted in 2008. This hearing
disorder is complex, as evidenced by the many names, explanations, and
classifications of the disorder, which has also been called Dysynchrony and Central
Auditory Neuropathy. Due to the involvement of the cochlear portion of the 8th
cranial nerve (and sometimes the vestibular portion as well), this disorder
technically can be considered a subset of SNHL, but is often differentiated due to
dissimilar function and test results.
Children presenting
with this hearing loss may have sporadic windows of hearing or near normal hearing
and at other times may not respond to sound at all. The children that do respond to
speech will often will have difficulty distinguishing one sound from another and
trouble understanding speech clearly. In some cases, ANSD causes only mild hearing
difficulties and is only a problem in noisy situations. In the majority of cases,
however, it leads to significant hearing loss. Due to the variability in auditory
performance, habilitation recommendations are based on speech and language
development and can range from audiological monitoring to hearing aid fitting and
cochlear implantation.
The causes of ANSD are unknown, but
children who are born prematurely or have a family history of the condition are at
higher risk for it. Symptoms can develop at any age, but most kids with ANSD are
born with it and diagnosed in the first months of life. As ANSD becomes better
understood, it is diagnosed more frequently and now accounts for about 10% to 15% of
cases of hearing loss. Case reports suggest that auditory neuropathy may be
associated with other types of neuropathies, such as Charcot-Marie-Tooth,
Friedrich’s Ataxia, and Refsum syndrome, as well as associated with AIDS infection.
[Hain: 2017]
Central Hearing Loss and Central Auditory Processing Disorder
In central hearing loss, the central nervous system, specifically the brain, encounters difficulty processing speech. Even when sound is effectively transmitted through the outer, middle, and inner ear, the brain is unable to properly interpret these signals. Central hearing loss therefore can also be considered a central auditory processing disorder. Auditory processing disorder is type of learning disability that affects many different people, however the problem itself is not well understood. Affected people may have difficulty understanding speech in certain situations, for example when there is significant background noise or when they are already attending to other auditory stimuli. This is not the same as functional hearing loss, in which an individual with normal hearing mechanisms may not respond to auditory cues due to behavioral or psychological differences. The functional difference between a central auditory processing disorder and an auditory neuropathy (above) can be slim, although test results can help differentiate the disorders.
In this disorder, routine hearing tests may be normal, reflecting the normal function of the outer, middle, and inner ear and 8th cranial nerve, however the individual may still struggle to understand and interpret speech. Testing for this condition is difficult, so diagnosis typically requires a person who has experience recognizing it. In children, awareness of this condition can help increase needed supports, such as limiting background noise to enhance classroom performance and learning. Frequency modulation auditory trainers have been used for children with central auditory processing problems.
Unilateral Hearing Loss
Children with unilateral (one-sided) hearing loss are at risk for academic failure, experience considerable difficulty in understanding speech in a background of noise, experience trouble with localization (with resulting safety issues), and appear to exhibit more behavioral problems in school. Despite these challenges, clinical practice in terms of intervention for this population is variable.[Fitzpatrick: 2010] Children at greatest risk for educational problems exhibit a specific profile that includes, early age of onset, perinatal and/or postnatal complications, severe-to-profound sensorineural impairment, and right ear impairment. Children with unilateral hearing loss can be helped in the academic setting through careful classroom management and amplification.
- Children with unilateral hearing loss should be given seating preference and, when a choice of classrooms is available, the child should be placed in the classroom with the least amount of ambient noise and reverberation. Proper illumination can help the child to augment his/her understanding through visual cues and speech reading. Teachers should be informed that the child might have difficulty with speech understanding and localization especially under noisy conditions. In-service training may help teachers to recognize potentially frustrating educational settings and provide appropriate solutions.
- Students with unilateral hearing loss may also benefit from using frequency modulation (FM) auditory trainers in the classroom setting. The main advantage of FM auditory trainers is their ability to transmit the speaker's voice without the attenuation caused by physical distance and background noise. Such a system may be particularly helpful for students who are experiencing difficulty in the academic setting or have special listening problems that cannot be solved by changes in the classroom environment.
- Fitting the affected ear for a hearing aid may enhance communication outside the classroom setting.
- Children with unilateral hearing loss should be monitored carefully for conductive hearing loss from otitis media with effusion in either ear and for progressive hearing loss. Several authors suggest that these children should receive annual audiologic evaluations and, particularly when the hearing loss is progressive, more periodic evaluations may be desirable.
- Parents and teachers should be counseled that these children might encounter specific dangers in common situations such as crossing busy streets or riding a bike in heavy traffic. They should also be encouraged to provide protection from high noise levels.
Hereditary Non-Syndromic Hearing Loss
Over 100 genes are predicted to cause hereditary forms of nonsyndromic hearing loss (hereditary forms of hearing loss not associated with a broader genetic syndrome). As the chromosomal locations (loci) of the various genes responsible for nonsyndromic hearing loss are discovered, they are given specific designators based on their inheritance pattern and their order of discovery. Loci of genes causing X-linked forms of hearing loss are given the designation DFN and then numbered sequentially (DFN1, DNF2, DFN3...). Autosomal dominant loci have DFNA as their common designator (DFNA1, DFNA2, DFNA3...) and autosomal recessive loci have DFNB as their common designator (DFNB1, DFNB2, DFNB3...).
Different mutations within the same gene may cause different kinds of nonsyndromic or syndromic hearing loss. Different mutations in the Connexin 26 gene, for example, can lead to a dominantly inherited form of hearing loss associated with the DFNA3 locus on chromosome 13q12 or an autosomal recessive form of hearing loss associated with the DFNB1 locus at the same chromosomal location. Some specific mutations may cause both a syndromic form of hearing loss and a nonsyndromic form. Mutations in the Pendred syndrome gene (PDS), for example, cause both Pendred syndrome (sensorineural hearing loss and goiter) and an autosomal recessive form of nonsyndromic hearing loss associated with the DFNB4 locus on chromosome 7q31.
Resources
Information & Support
For Professionals
Hereditary Hearing Loss Homepage
Provides an up-to-date overview of the genetics of hereditary hearing impairment for researchers and clinicians working in
the field. This site lists data and links for all known gene localizations and identifications for nonsyndromic hearing impairment.
For syndromic hearing impairment, only a few of the most frequent forms are covered.
National Institute on Deafness and Other Communication Disorders
A National Institute of Health site; it offers related health information, as well as information about research and research
funding.
American Speech-Language-Hearing Association
Information for professionals working in audiology, speech-language pathology, and the speech and hearing sciences. Advocate
for people with communication disabilities.
Deafness, autosomal recessive (OMIM)
Information about clinical features, diagnosis, management, and molecular and population genetics; Online Mendelian Inheritance
in Man, authored and edited at the McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University School of Medicine
Deafness, autosomal dominant (OMIM)
Information about clinical features, diagnosis, management, and molecular and population genetics; Online Mendelian Inheritance
in Man, authored and edited at the McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University School of Medicine
Dizziness-and-Balance
Website authored by Timothy Hain, MD, with detailed information about Auditory Neuropathy and related information.
For Parents and Patients
Learning About Hearing Loss - A Roadmap for Families (NCHAM) ( 347 KB)
347 KB)
Graphic representation of the path to learning about hearing loss, from a positive newborn hearing screen to 6 months of age;
National Center for Hearing Assessment and Management.
Learning about Hearing Loss - A Roadmap for Families (NCHAM) (Spanish) ( 287 KB)
Spanish language graphic representation of the path to learning about hearing loss, from a positive newborn hearing screen
to 6 months of age; National Center for Hearing Assessment and Management.
Practice Guidelines
American Academy of Family Physicians, American Academy of Otolaryngology-Head and Neck Surgery, and American Academy of Pediatrics
Subcommittee on Otitis Media With Effusion.
Otitis media with effusion.
Pediatrics.
2004;113(5):1412-29.
PubMed abstract
American College of Medical Genetics Newborn Screening Expert Group.
Genetics Evaluation Guidelines for the Etiologic Diagnosis of Congenital Hearing Loss. Genetic Evaluation of Congenital Hearing
Loss Expert Panel. ACMG statement.
Genet Med.
2002;4(3):162-71.
PubMed abstract / Full Text
Guideline reaffirmed by the ACMG in 2005
Patient Education
Let's Talk About... Hearing and Testing (English) ( 143 KB)
Fact sheet with a brief overview and types of tests; Intermountain Healthcare.
Services for Patients & Families in Nevada (NV)
| Service Categories | # of providers* in: | NV | NW | Other states (3) (show) | | NM | RI | UT |
|---|---|---|---|---|---|---|---|---|
| Pediatric Otolaryngology (ENT) | 5 | 1 | 11 | 7 | 10 | |||
For services not listed above, browse our Services categories or search our database.
* number of provider listings may vary by how states categorize services, whether providers are listed by organization or individual, how services are organized in the state, and other factors; Nationwide (NW) providers are generally limited to web-based services, provider locator services, and organizations that serve children from across the nation.
Helpful Articles
PubMed search for hearing loss or deafness in children, last 1 year
Bess FH, Tharpe AM.
An introduction to unilateral sensorineural hearing loss in children.
Ear Hear.
1986;7(1):3-13.
PubMed abstract
Bess FH, Tharpe AM.
Performance and management of children with unilateral sensorineural hearing loss.
Scand Audiol Suppl.
1988;30:75-9.
PubMed abstract
Davidson J, Hyde ML, Alberti PW.
Epidemiologic patterns in childhood hearing loss: a review.
Int J Pediatr Otorhinolaryngol.
1989;17(3):239-66.
PubMed abstract
Doyle KJ, Ray RM.
The otolaryngologist's role in management of hearing loss in infancy and childhood.
Ment Retard Dev Disabil Res Rev.
2003;9(2):94-102.
PubMed abstract
Fitzpatrick EM, Durieux-Smith A, Whittingham J.
Clinical Practice for Children with Mild Bilateral and Unilateral Hearing Loss.
Ear Hear.
2010.
PubMed abstract
Johnson DL, McCormick DP, Baldwin CD.
Early middle ear effusion and language at age seven.
J Commun Disord.
2008;41(1):20-32.
PubMed abstract
Lous J, Burton MJ, Felding JU, Ovesen T, Rovers MM, Williamson I.
Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children.
Cochrane Database Syst Rev.
2005(1):CD001801.
PubMed abstract
McKay S, Gravel JS, Tharpe AM.
Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss.
Trends Amplif.
2008;12(1):43-54.
PubMed abstract
Current hearing technology options for children with minimal or mild bilateral hearing loss or unilateral hearing loss are
reviewed.
Paradise JL, Feldman HM, Campbell TF, Dollaghan CA, Colborn DK, Bernard BS, Rockette HE, Janosky JE, Pitcairn DL, Sabo DL,
Kurs-Lasky M, Smith CG.
Effect of early or delayed insertion of tympanostomy tubes for persistent otitis media on developmental outcomes at the age
of three years.
N Engl J Med.
2001;344(16):1179-87.
PubMed abstract
Paradise JL, Feldman HM, Campbell TF, Dollaghan CA, Rockette HE, Pitcairn DL, Smith CG, Colborn DK, Bernard BS, Kurs-Lasky
M, Janosky JE, Sabo DL, O'Connor RE, Pelham WE Jr.
Tympanostomy tubes and developmental outcomes at 9 to 11 years of age.
N Engl J Med.
2007;356(3):248-61.
PubMed abstract
Page Bibliography
American Academy of Family Physicians, American Academy of Otolaryngology-Head and Neck Surgery, and American Academy of Pediatrics
Subcommittee on Otitis Media With Effusion.
Otitis media with effusion.
Pediatrics.
2004;113(5):1412-29.
PubMed abstract
American College of Medical Genetics Newborn Screening Expert Group.
Genetics Evaluation Guidelines for the Etiologic Diagnosis of Congenital Hearing Loss. Genetic Evaluation of Congenital Hearing
Loss Expert Panel. ACMG statement.
Genet Med.
2002;4(3):162-71.
PubMed abstract / Full Text
Guideline reaffirmed by the ACMG in 2005
Bess FH, Tharpe AM.
An introduction to unilateral sensorineural hearing loss in children.
Ear Hear.
1986;7(1):3-13.
PubMed abstract
Bess FH, Tharpe AM.
Performance and management of children with unilateral sensorineural hearing loss.
Scand Audiol Suppl.
1988;30:75-9.
PubMed abstract
Davidson J, Hyde ML, Alberti PW.
Epidemiologic patterns in childhood hearing loss: a review.
Int J Pediatr Otorhinolaryngol.
1989;17(3):239-66.
PubMed abstract
Doyle KJ, Ray RM.
The otolaryngologist's role in management of hearing loss in infancy and childhood.
Ment Retard Dev Disabil Res Rev.
2003;9(2):94-102.
PubMed abstract
Fitzpatrick EM, Durieux-Smith A, Whittingham J.
Clinical Practice for Children with Mild Bilateral and Unilateral Hearing Loss.
Ear Hear.
2010.
PubMed abstract
Gifford KA, Holmes MG, Bernstein HH.
Hearing loss in children.
Pediatr Rev.
2009;30(6):207-15; quiz 216.
PubMed abstract
Hain H.
Auditory Neuropathy.
Hain; (2017)
http://www.dizziness-and-balance.com/disorders/hearing/aud_neuropathy..... Accessed on 1/2018.
Johnson DL, McCormick DP, Baldwin CD.
Early middle ear effusion and language at age seven.
J Commun Disord.
2008;41(1):20-32.
PubMed abstract
Lous J, Burton MJ, Felding JU, Ovesen T, Rovers MM, Williamson I.
Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children.
Cochrane Database Syst Rev.
2005(1):CD001801.
PubMed abstract
McKay S, Gravel JS, Tharpe AM.
Amplification considerations for children with minimal or mild bilateral hearing loss and unilateral hearing loss.
Trends Amplif.
2008;12(1):43-54.
PubMed abstract
Current hearing technology options for children with minimal or mild bilateral hearing loss or unilateral hearing loss are
reviewed.
Paradise JL, Feldman HM, Campbell TF, Dollaghan CA, Colborn DK, Bernard BS, Rockette HE, Janosky JE, Pitcairn DL, Sabo DL,
Kurs-Lasky M, Smith CG.
Effect of early or delayed insertion of tympanostomy tubes for persistent otitis media on developmental outcomes at the age
of three years.
N Engl J Med.
2001;344(16):1179-87.
PubMed abstract
Paradise JL, Feldman HM, Campbell TF, Dollaghan CA, Rockette HE, Pitcairn DL, Smith CG, Colborn DK, Bernard BS, Kurs-Lasky
M, Janosky JE, Sabo DL, O'Connor RE, Pelham WE Jr.
Tympanostomy tubes and developmental outcomes at 9 to 11 years of age.
N Engl J Med.
2007;356(3):248-61.
PubMed abstract